|
Hip Surface Replacements & Total Hip Replacements |
|
![]()
| Background
Hip replacement surgery has been around since the early 1960s. Sir John Charnley experimented in the early 1950s, and he used a small (22 mm) stainless steel ball on a stem in 1962 that he inserted into the femur (hip) bone to replace the femoral head (ball). He then inserted a high-density plastic socket to replace the acetabular (socket) side of the hip joint. Both were secured with a self-curing acrylic polymer known as bone cement. |
|
Today, the modular balls are made of a cobalt-chrome metal alloy or a ceramic material, and some of the components are press-fit and do not require bone cement. The procedure remains basically the same: (1) the femur bone is amputated to remove the femoral head; (2) the femoral canal is reamed-out for insertion of the stem; (3) an acetabular socket is affixed to the socket side of the hip; and (4) the ball joint is inserted into the acetabular socket. This is known as a total hip replacement, or more correctly, total hip arthroplasty (THA). |
image from www.wmt.com (Click on image to enlarge) |
|
image from www.jri-oh.com (Click on image to enlarge) |
image from www.jri-oh.com (Click on image to enlarge) |
|
The acetabular socket used in THA is normally lined with a high molecular weight polyethylene (sometimes the liner is ceramic). A metal or ceramic ball is attached to the stem and rotates within the socket. Fine particulate debris is produced from the wearing process of the ball against the liner that leads to tissue reaction. The body’s immune system attacks the debris, and consequently, attacks the adjacent bone supporting the THA device, leading to bone loss and a loosening of the device. This bone loss is known as osteolysis. To lessen the amount of wear, a small ball (approximately 30 mm) is used; however, the small size of the ball makes the joint less stable and increases the risk of dislocation in certain circumstances. The loosening of the THA device requires revision surgery in which a larger diameter stem must be inserted in the femoral canal. Depending on the age and activity of the patient, multiple revision surgeries may be necessary throughout a patient’s life. A young (under 60), active individual can expect only 10 – 15 years before needing revision surgery. Revision surgery can be complex and costly. The lifespan of a THA device is clocked in miles rather than years. (Note: Wright Medical Technology, Inc. has developed a large femoral head using metal-on-metal technology (see Hip Surface Replacement below) that reduces the risk of dislocations and osteolysis in THRs. The large head THR has received FDA approval and is actively being marketed.) |
| Hip
Surface Replacements
Although it was experimented
with and attempted in the 1960s, metal-on-metal “resurfacing” of
the femur and acetabulum was abandoned because of loosening of the
fittings. With the refinement of acrylic fixation and its very
successful use with the THA stem, interest in hip resurfacing was renewed,
and it was subsequently used in several countries in the 1970s. (See History
of Hip Resurfacing.) Resurfacing has the advantage of preserving the femoral bone stock (and marrow contained in the femur). It also has the advantage of easy future revision to THA if it becomes necessary. Since the femur is persevered and not amputated in the initial hip surface replacement surgery, it is available to support a THA stem should revision become necessary. Maintaining the integrity of the femur bone also aids in the mechanical transfer of weight and stress in a more natural manner. Where THA patients often experience thigh pain, recipients of hip surface replacements avoid that particular discomfort. |
|
image from www.jri-oh.com (Click on image to enlarge) |
image from www.jri-oh.com (Click on image to enlarge) |
|
Using a metal acetabular socket as
well as a metal cap over the femur head (metal-on-metal) eliminates the
polyethylene debris produced in THA.
The metal wear debris from a hip surface replacement produces
smaller particles than polyethylene wear debris.
The inflammatory response to metal debris is considerably less than
that from polyethylene debris. It is believed that the body can partially dissolve and expel
metal since it is a naturally occurring substance in the body.
There is concern by some of the toxicity of metal, but there is
currently no definitive evidence that metal ions cause cancer.
Since a metal surface does not wear as readily as a polyethylene
lining, a larger ball (approximately 38-51 mm) can be used that adds stability
to the joint and reduces the danger of dislocation. |
images from www.wmt.com & www.jri-oh.com (Click on images to enlarge) |
|
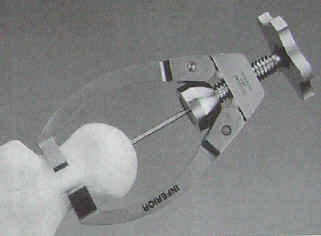
The surgery time for hip
surface replacement is slightly longer than that for THA.
The attachment of the acetabular socket is basically the same.
It is press-fitted and does not require bone cement.
The attachment of the cobalt-chrome cap requires a more precise
alignment, and it takes slightly longer to fit.
The hole for the pin insertion must be aligned and drilled, and the
dome of the femoral head must be ground and shaped to fit the cap.
Some bone cement is used to affix the cap, but the interior surface
of both the cap and the socket is such that bone grows into the relief
surface to grip the device. |
|
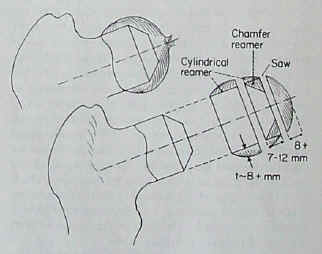
The following images are from an Instructional Lecture delivered at an International Symposium in Fukuoka, Japan on March 16, 1996 by Harlan C. Amstutz, Peter Grigoris, and Frederick J. Dorey entitled "Evolution and future of surface replacement of the hip." Journal of Orthopaedic Science. J Orthop Sci (1998) 3:169-186.
Superimposed hemisurface. Pin centering guide. Cylindrical reamer.
Saw cutoff guide and oscillating saw. Chamfered reamer. Femoral head bone preparation. (Click on images to enlarge) |
|
Risks involved in the hip
surface replacement surgery are the same as the risks involved in any
major surgery. Risks specific to the hip surface replacement involve the
potential for cracking in the neck of the femur bone due to the drilling
of the guide hole through the neck for the support pin in the metal cap,
and also a negative reaction of the femur head to dislocation and being reshaped to fit
the metal cap leading to the development of avascular necrosis (bone
death)--often referred to as AVN--due to a disruption of blood circulation
to the femur head and neck (see AVN Risk).
In such instances, a THA could easily be performed to correct the
problem. Hip surface replacement in the United States has been pioneered by Harlan C. Amstutz, M.D. at the Joint Replacement Institute in Los Angeles, CA. For years, a hip surface replacement in the United States has been labeled an “investigative device” by the Food and Drug Administration (FDA). The longest study has been conducted by Wright Medical Technology, Inc. under the product name of CONSERVE ® Plus Total Resurfacing Hip System. The clinical trials have proceeded for a number of years, and they are nearing their end. They have involved nine surgeons across the country in California, Florida, Texas, Maryland, North Carolina, Ohio, and in the Pacific Northwest. Corin Medical, Ltd. of the United Kingdom has also begun an FDA study in the United States using the Cormet 2000 device. Click here to read the 2-6 year follow up report of the first 400 CONSERVE ® Plus hips. In Europe, the Birmingham Hip Surface Replacement System (BHR) has been in use for many years. Smith & Nephew Inc., manufacturer of the BHR, applied for FDA approval, and perhaps due to the long record of use in Europe, they obtained FDA premarket approval to begin commercial distribution of their device in the United States on May 9, 2006 (see FDA approval letter and FDA announcement). Because the BHR was not previously used in the United States, the number of American surgeons qualified to use it was limited due to the fact that they had all been participating in the Wright and Corin studies; however, that is destined to change with the FDA approval obtained by Smith & Nephew. |
| My
Experience
Pre-surgery | Surgery | 0 - 3 Months | 4 - 7 Months | 8 - 11 Months | 1 Year | Revision Surgery | Revision Recovery | 2 Years Post-Revision | 3 Years Post-Revision | 5 years Post-Revision It was an injury in the mid 1980s while playing volleyball followed by years of subsequent daily jogging that led to the loss of cartilage in my hip—that and a predisposition to arthritis inherited from my parents. In 1998 an orthopedic surgeon viewed my X-rays and told me that I would need a hip replacement. |
|
In addition to the arthritis found in the joint, the circled area shows the loss of cartilage at the top of the damaged hip where the bone was close to touching in 1998. (It’s amazing that such a small area could cause such pain.) The arrow pointing to the joint of the “healthy” hip shows how the layer of cartilage should appear (although the healthy hip also shows evidence of arthritis). |
1998 X-ray (Click on image to enlarge) |
|
When I was given the prognosis,
I endeavored to learn as much as I could about hip replacements.
The more I learned, the more I wanted to avoid the surgery for as
long as possible. The thought
of numerous revision surgeries throughout the remainder of my life and the
danger of dislocation and the
movement restrictions necessary to avoid
dislocation were enough of an incentive to make me change my habits. I immediately stopped jogging and playing volleyball,
and I began taking supplements of chondroitin, gloucosamine, and MSM (the
building blocks of cartilage). Through such efforts, I was able to slow the progress of the degeneration; however, subsequent X-rays revealed that the cartilage loss still progressed but at a slower rate. |
|
2000 X-ray (Click on image to enlarge)
|
2001 X-ray (Click on image to enlarge) |
|
Also during this time, I
learned about the hip surface replacement, and this knowledge helped eased
some of my fears about dislocation, activity restrictions, and the
longevity of the artificial hip. Even
though it is on the other side of the country, I was prepared to travel to
the Joint Replacement Institute in Los Angeles to have the surgery
performed by Dr. Harlan Amstutz, Dr. Thomas Schmalzried, or Dr. Paul
Beaulé.
However, when I called the FDA to inquire about the status of the
clinical trials, I was referred to Wright Medical Technologies (the manufacturer of
the device), and I learned of other physicians closer to me who were also
participating in the clinical trials.
The two closer physicians were Dr. Michael Mont at Johns Hopkins University,
Sinai Hospital in Baltimore, Maryland, and Dr. Victor M. Goldberg at the University Hospitals
of Case Western Reserve in Cleveland, Ohio. (Other physicians participating
in the FDA trials include Dr. Ed Sparling in Vancouver, WA; Dr.
Harold Boyd in Salem, OR; Dr. Mike Grecula in Galveston, TX; Dr. Thomas Parker
Vail in Durham, NC; and Dr.
William Kennedy in Sarasota, FL.) Since Dr. Goldberg is only two hours away, I arranged to have him perform the surgery. Prior to the surgery we discussed all the potential risks of hip resurfacing and surgery in general, and the surgery was performed on December 3, 2002 in an operation that lasted approximately three hours. I left the pre-op room at 5:15 p.m., and I was unconscious before I even arrived in the operating room. General anesthesia was administered, so I was unconscious for the entire operation. I awoke in my room at 11:00 p.m. (I have a quasi-conscious remembrance of the insertion of Foley catheter in the recovery room, as well as a rather painful remembrance of another occurrence, possibly when they moved me into my bed.) Upon awakening, I experienced no real discomfort. In fact, the first night was rather pleasant. I had an almost euphoric feeling most of the night that I attribute to the morphine I.V. The nurses attended to me hourly, checking my blood pressure and temperature, and my legs were secured so I could not move them. An intermittent pulsatile compression device (IPC) was placed around the calves of my legs that massaged them continually in a pleasant, rhythmic manner. Up my side and curving slightly over the buttocks, I had a ten inch incision secured with 32 staples. I remained in the hospital until December 7, 2002, and during that period, I experienced no real pain as long as I remained in bed. It was only when I got on or off the bed that I realized the potential for hurt caused by the trauma of the surgery. The patient-controlled analgesia (PCA)--morphine I.V. pump--remained attached during the first two days of hospitalization. Later, it was removed in place of oral pain medication. At the same time the Foley catheter was removed. Physical therapy began the day after surgery, and it consisted of sitting on the edge of the bed, standing, and walking to the door. Subsequent days involved exercises, the use of crutches, walking longer distances, and climbing stairs. (Stair climbing proved to be one of the easiest feats to perform.) I was released to my home with visiting nurses and home therapy ordered by Doctor Goldberg. The near two-hour car ride home was a living hell, and upon exiting the car, I swore I’d never ride in one again. After a few weeks, I changed my mind about automotive travel and climbed back into a car--as a passenger, of course. Visiting nurses came three times a week to monitor my blood level due the the Coumadin/Warfarin (blood thinner) I was prescribed, and these visits continued until New Years Day when a daily child's aspirin was substituted for the Coumadin/Warfarin. A visiting nurse was also the one who removed my staples after two weeks. A physical therapist visited three times to continue the stretching exercises, but she was unable to do more with me until I was able to place 100% of my weight on the operative leg. Because I live alone, I had a rotation of friends sleep over during the first five nights after my return home. Originally, I thought I could fend for myself, but the first day after surgery taught me that my weakness had become too extreme for that. It proved to be a good decision on my part because the first few nights were extremely painful and required the assistance of others. At home I experienced much more pain than I had known in the hospital. Some of the pain was a result of my sitting upright in a chair for up to 18 hours a day the first few days, but this pain seemed to subside once a recliner was moved into my living room and I was able to recline and sleep during the day. Within four days of returning home, I could almost completely refrain from taking any pain medication; however, in the first few days, I was taking the full dosage every four hours—day and night. (See Pain Medications.) Sleeping in a bed also proved problematic in the first few days after returning home. Besides the pain of getting on and off the bed, I experienced a lot of lower back discomfort from sleeping immobile on my back all night long. After three days at home, I was able to get on and off the bed myself with minimal discomfort (using a garbage bag to slide on and off the bed), but sleeping on my back still proved uncomfortable after a few hours. I looked forward to a time when I could again sleep on my side and stomach. Most people have this surgery because the pain of walking has become so excruciating for them that they can’t stand it anymore. As a result, the surgical pain and the pain of recovery is less than or equal to what they had been experiencing prior to the surgery. In the eight months leading up to my surgery, the pain had diminished, but my leg remained deformed without any range of motion. Because of my lack of excruciating pre-surgical pain, I found the discomfort of the surgery more than I had anticipated—or at least more than what I had been told by others to expect. Even though the pain seemed overwhelming at the time, it was short-lived, and I managed to endure it. |
|
I was restricted to placing only 25% of my weight on the operative leg for the first eight weeks, and I used crutches or a walker until I returned for my post-op examination on January 27, 2003. At that time, the doctor wrote me a prescription to start physical therapy. He also advised me to begin swimming, but not until I had completed at least one week of physical therapy. He stated that I could sleep on my side and stomach, and he even allowed me to begin sleeping on the operative side, but that still proved a little uncomfortable. |
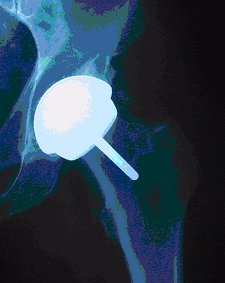
January 2003 X-ray (Click on image to enlarge) |
|
January 2003 X-ray (Click on image to enlarge) |
When I asked about returning to work, he told me to come back in six weeks and "we'd talk about it." That was something I was not prepared to argue with because I really did not feel ready to go back to work just then. Since it was winter, there were a lot of travel concerns I had about commuting to and from my job, and I did not want to risk falling and damaging the new implant. I had a dentist appointment scheduled for February 7th, but Dr. Goldberg advised me to postpone it and reschedule it for sometime in April. Evidently, he was still concerned about infection, and he didn't want me to take any unnecessary risks. |
|
I began physical therapy the day after my doctor's appointment. After two months of limited activity, the muscles in my operative leg were slow to respond. I drove myself to the therapy, and that was an experience in itself. That was my first driving experience since my surgery. Because my car is small and my operative leg is my right leg, it took some maneuvering to just get into the car. I couldn't move the leg from the gas pedal to the brake pedal, so I was forced to drive with two feet. I also had to recline the seat quite a bit, which made seeing over the dashboard a challenge. Needless to say, I was menace on the road. Eventually, I adapted to my new driving technique, and it became a lot easier to get in and out of the car. I was also able to reduce the incline of the seat as I progressed through the therapy. My physical therapy involved a number of strengthening exercises (i.e. leg raising exercises) which I perform at the therapy sessions as well as once or twice a day at home during my "off days." (The therapist informed me that I would always have to be doing the exercises he taught me for as long as I had my prosthetic hip, and I would have to find a way to incorporate them into my normal post-op life.) Going to therapy two days a week, I progressed from two crutches to one crutch after the first week and from one crutch to a cane after the second week. After the third week I began walking without the cane at home but still used it when I went out. It took a lot of concentration and deliberate effort to walk without limping when I didn't use the cane, but it became easier as time went by. It was almost like learning to walk all over again. I also started swimming at the YMCA after two weeks of therapy. (I would have started after the first week, but I had to contend with a head cold--my resistance to germs and infection after my surgery was practically nil.) I had swum regularly prior to surgery, so I already felt comfortable in the water; however, when I first entered the water, I was far from comfortable. In the water, the hip felt like a foreign object in my body (which it was), but something about the water amplified the feeling. It felt like it could easily slip out of joint if I kicked too hard, but soon that feeling passed. By the third length of the pool, it started to feel normal, and by the third lap, it was just like my old hip. I managed to swim my usual half mile without a problem. Of course, I had to contend with upper body stiffness the next day from muscles that hadn't been used for over two months. I found swimming to be excellent therapy. Besides swimming a half mile using an Australian crawl stroke, I also used a kick board to do additional laps, and I would walk back and forth through water up and down a swimming lane. I did this twice a week right after I left my physical therapy sessions because the therapy finish times coincided with the lap swim start times at the YMCA. On my "off days" I would go to a mall and walk (one to one and a quarter miles) and then go to the YMCA to use some of the Nautilus exercise equipment to strengthen my upper body. I returned to Dr. Goldberg again on March 10, 2003. He told me to put away the cane, and he released me to do more strenuous exercises to build up the strength in my leg. His recovery plan had been basically this: eight weeks of rest for the incision to heal and for the bone to grown into the implant; six weeks of physical therapy and swimming in order to learn to walk again; followed by a more intense exercise program designed to restore strength to the hip and leg. These intense exercises involved the use of weights and Nautilus equipment along with a continuation of the swimming and walking. He identified which pieces of exercise equipment he thought would be good (e.g. elliptical trainer, treadmill, and various leg weight machines) and which ones I should avoid (e.g. leg press machines and the Stairmaster). He specifically prohibited me from running and jumping. In addition to prescribing lots of activity and exercise, he released me to return to work. I put away the cane (although it was a struggle not to limp without it), and I proceeded to engage a more strenuous exercise program. I addition to the routine exercises I learned in physical therapy, I began a daily schedule of 20 minutes on an elliptical trainer, followed by 15 minutes on a treadmill, followed by 10 minutes on a stationary bicycle, followed by leg weight training on Nautilus machines. Oh yes, I also continued to swim. Six days after my doctor visit, I experienced a sharp pain in my hip while walking out of a gas station, and that was enough to put me back on the cane for two additional weeks. I decided that I had overdone the exercise bit, so I scaled it back to every-other-day workouts. Also, I only did one thing on my workout day be it swimming or bicycling or weight training or whatever. After two weeks, I was ready to give up the cane, and this time I was truly ready because I could then walk without struggling and without limping. I found that I was merely carrying the cane and not really using it. I had read that you should use a cane until you can walk without a limp, and I learned the wisdom of what I had read. You eventually get to that point where your body is ready to give up the cane--and you don't arrive at that point until your body is ready. There's no sense in forcing the issue. The bottom line is that I should have been content to make slow steady progress and not push it so hard. A valuable lesson was learned, but it was learned the hard way. By the fourth month post-op, spring had arrived, and I was outside engaging in a lot of springtime activities like cutting the grass and working around the house and yard. I found that such normal activities--like washing the car and walking on the uneven ground around my yard--were also good therapy. The hip would still get sore on days when I worked it too hard, but all-in-all, it was feeling pretty good. I pulled my boat out of storage, and was able to climb up and down the ladder and all over the boat as I cleaned it and prepared it for summer fun. At that time, I was still careful about how I moved and walked, but it was becoming much less of a conscious concern. When the muscles were relaxed, the hip joint would painlessly "thunk and clunk" when I'd move suddenly, so there was always that reminder that I had a prosthetic hip. I would described the sensation as the same thing I'd experience in my car when I pulled my boat on the trailer as the ball joint on the trailer hitch would bump inside the trailer tongue coupling. As the "sensation" in the car would remind me not to do anything stupid because I was pulling a trailer behind me, the "sensation" in my body would remind me not to do anything stupid because of my prosthetic hip. Every morning I started my day with the exercises I had learned in physical therapy, and I continued my workout routine at the YMCA every other day. I was progressing confidently and painlessly. Then when I was five months post-op, I began experiencing a return of the pain in my hip. It started as an ache while walking when I put weight on the leg. It was an ache that increased as I walked as if it were building to a sharp, stabbing pain if I made the mistake of walking too far. As a result, I started limiting the distance I'd walk my dog each night, and I curtailed my workouts at the YMCA, but it didn't seem to matter. Within a week, I was getting a jabbing pain in my hip even when I walked a short distance. The hip had become very "tender" to certain movements and having weight applied to it. I called the doctor's office, but they didn't seem overly concerned about it. They told me that I had probably just "overdone it," and they told me to rest. Although I didn't feel like I had overdone it, I took their advice. I scaled back my activities, and the pain subsided dramatically. Evidently, I had tried to returned to my normal pre-op routines a little too soon, and my hip wasn't quite ready for all my frantic movements and activity. Just by slowing down the pace at which I walked seemed to make a world of difference. I also noticed that my range of motion had greatly increased, and I speculated that the muscles, ligaments, and tendons had needed time to adjust. Perhaps they had been the source of my newfound pain. |
|
June 2003 X-ray (Click on image to enlarge) |
I returned to Dr.
Goldberg on June 9, 2003 for my six-month follow-up exam. The
X-rays looked good and nothing appeared out of the ordinary.
He said that he was a little concerned about the tenderness and
achiness I was experiencing because, at six months, I should not be
having any significant pain. He speculated that it could be some
residual soft tissue damage that had yet to repair itself, and he
took a wait-and-see approach.
I had already resigned myself to the fact that I was a slow healer--it took me a year to completely recover and lose all the pain from root canal--so I decided to give the hip at least that long before becoming really concerned about it. In the meantime, I decided to take it slow and easy--well, as slow and easy as I was able to manage. I went on vacation to the shore a few days after seeing the doctor, and I found myself windsurfing again and boogie boarding in the ocean waves. I wanted to see if I could do it, and I came through with flying colors (see Windsurfing Article). I also found walking the beach in the sand to be very therapeutic. And besides windsurfing and boogie boarding, I was able to sail my boat without any major problems. |
When I reached my eight month anniversary, I noticed some marked improvements. I was able to effortlessly climb stairs where only a month earlier I would still feel some strain in the hip. The hip's range of motion had also greatly improved, and I was able to reach down to my foot a lot easier. I would still experience some slight tenderness or weakness in the hip from time to time and a mild ache now and then, but it was nothing like before. At nine months, the hip joint seemed to increase in tenderness, and I noticed an increase in pain. The pain was not that significant, and it did not keep me from my normal activities. It was just mentally disconcerting because I did not expect to be experiencing any pain or weakness in the leg at that stage. I also noticed that the mild achiness of the hip extended down the leg and into the shin area that made me question if the sciatic nerve might not be playing a role in my discomfort and leg weakness. But then one day the pain became extreme enough that it made it hard to walk. It was very reminiscent of the pain I had experienced prior to surgery. I also was experiencing a low-grade fever, so I thought an infection might have developed in the hip. (For symptoms of possible implant failures see Implant Failure Symptoms.) I immediately called the doctor, and he asked me to come into his office. After looking at the X-rays, he assured me that there was no infection, but he said that he worried that a pending stress fracture might be developing. We also discussed the potential of avascular necrosis (AVN) forming at the end of the femur. (10,000 to 20,000 people develop AVN every year, mostly men between the ages of 30 to 50 years, and AVN normally develops close to the joint.) Because the end of the femur is not amputated in resurfacing, as in a total hip replacement, it is still possible to develop AVN after resurfacing. He also told me that I would definitely know if either of these conditions had developed by the pain that would result. Since the pain seemed to have subsided by the time of the office visit, he decided to take a wait-and-see approach. If the stress fracture or AVN diagnosis proved to be true, the only recourse would be revision surgery to a total hip replacement. He did assure me that he would use the new large femoral head THA that would allow me a greater activity level with less chance of dislocation, but that seemed a small consolation in light of having to again undergo all the pain and trauma of surgery. After a few days, I convinced myself that the pain had resulted more from tendon or ligament inflammation. Having dealt with inflammation in the plantar fascia of my foot, I knew how easily tendons and ligaments can become inflamed and how slow they are to heal. The pain in my hip behaved similarly to the pain I had experienced before in my foot. If not an inflammation of a tendon or ligament, I also suspected inflammation of the illiopsoas muscle (see Hip & Thigh Muscles). Either way, I convinced myself that the diagnosis of a pending stress fracture was probably just a "worse case scenario" about which the doctor had felt obligated to inform me. Within a week, the pain had completely disappeared, so I felt pretty confident that my own analysis of the problem had been correct. However, the pain did and would resurface sporadically, especially after I engaged in some strenuous activity, so I was left not knowing what to think. |
| One
Year
On November 12, 2003, I had my one-year follow-up exam. I arranged it a little early because I had booked a vacation to Cancun to celebrate my one-year anniversary in addition to my 50th birthday. I planned to windsurf, play volleyball, and do all the things I had to give up prior to my surgery. Unfortunately, things did not turn out the way I had planned. Circumstances couldn’t stop me from turning 50, but they stopped me from going to Cancun. |
|
November 2003 X-ray (Click on image to enlarge) |
Although my pain had decreased after my visit to the doctor two months earlier, the pain returned early October, and one week prior to my November 12th visit, I began walking with a cane to alleviate some of the weight bearing pain. The pain was not excessive, it was just a basic “soreness” that was present when I walked. It was especially evident during the first few steps after sitting or standing still. Except for one night, there was no aching or sharp pain when the leg was turned various ways. It was mainly weight bearing pain, and I could often alleviate it by walking a distance. There was less discomfort on long straight walks than there was with short quick steps or movements like you would make around the house or at work. I could lie on my back and do leg-raising exercises without pain. |
| Then to add insult to injury, I went to the dentist to have her check one of my teeth the day before my November 12th doctor visit, and she discovered that there was a major infection under a tooth with a root canal. Because of the deaden tooth, I could not feel the infection, but she speculated that it had been present for a long time, quite possibly at the time of my hip resurfacing one year earlier. The tooth was immediately removed, and I considered the possibility that the tooth had contributed to my hip problem. |
November 2003 X-ray (Click on image to enlarge) |
|
|
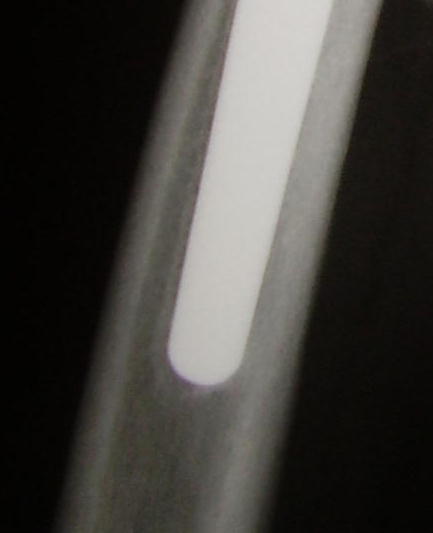
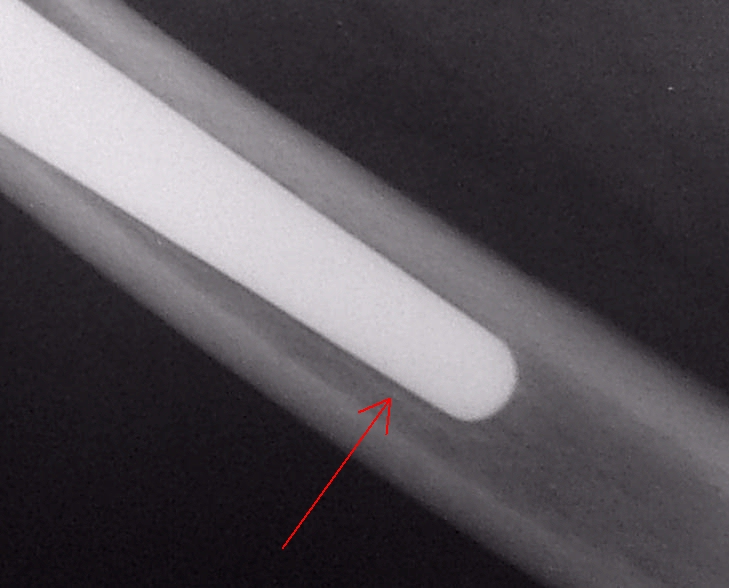
Unfortunately, my surgeon, Dr. Goldberg, did not share my belief that the tooth was causing my hip pain. Based on the X-rays, he thought the femur cap had become loose and was “wobbling.” He based that determination on a “line” that appeared in the X-ray along the guide pin (see black arrow in image). He also noted a jagged area of bone (what he referred to as "remodeling") that did not appear in previous X-rays (see red arrow in image). And he thought the femur cap might be rocking back and forth (see blue arrow in image). But still the issue of infection had to be addressed, and he scheduled me for a hip aspiration (i.e. the insertion of a needle into the hip capsule to remove and analyze the fluid for infection). |
| I had the hip aspiration on November 17, 2004. Instead of lying under the sun in the warm sand of Cancun, I was lying under an X-ray machine on a cold table while they inserted a needle into my hip through my groin. It was not pleasant, but I was able to survive it. Of course, I held tense every muscle in my body for about an hour during the procedure, and I was exhausted afterwards. The only really intense moment was when the X-ray technician lowered the equipment and accidentally hit the needle, shoving it right down to the bone. I'm lucky it didn't break off inside me. | |
| Dr. Goldberg felt that the femur cap had to be replaced with a THR stem using Conserve Total with BFH (Big Femoral Head) Technology. He said that he would use a 44 mm head that would fit into the acetabular cup already in place, and he suggested that I do it soon--possibly on the one year anniversary of my previous surgery. At first I was leaning toward the beginning of January 2004 because I had totally missed the holidays the previous year due to my recovery from resurfacing surgery, and I didn't want to miss them again. But then the pain became very intense, and it started disturbing my sleep. I was on crutches within a matter of days, and I was getting pain very similar to what I had experience immediately after surgery. It had become hard to get into and out of bed because of intense pain when I tried to lift or move my leg. I was forced to begin taking Vicodin to make the pain manageable at night. If I was going to experience pain similar to immediately post-surgery, I figured that I might as well go through the surgery again and at least have it be a healing pain. |
Wright Conserve Total with BFH Technology image from www.wmt.com |
|
The results of the hip aspiration concluded that
there was no infection in the hip, and that news made it possible to
proceed with revision surgery. Dr. Goldberg's final analysis in
his case notes was that there appeared "to be a stress fracture
with loosening of the femoral component . . . no evidence of any erosive
changes in the component itself, but there is stem motion," and he
concluded the need for a revision of the femoral component. He scheduled
the surgery for the second week of December 2003, and at that point I welcomed it due to the pain and
discomfort I was experiencing. But still, I felt like Bill
Murray in the movie Groundhog Day, reliving the same day over and
over again, and I wondered if the ordeal would ever have a happy ending.
Having the whole surgery experience fresh in my mind, I knew exactly what needed to be done to prepare myself and my home for the long recovery ahead; however, it proved a little more difficult because I had to accomplish it on crutches. Prior to my resurfacing surgery, I walked easily and had only to contend with an achy hip. With the failure of the implant, the pain was much more debilitating, and I was restricted in what I could do. I managed, however, to get through it, and everything was prepared to the extent it could be. Once again, the surgery season had arrived at the start of the winter season, which I found to be the best time of year to deal with the challenges of surgery and recovery. I normally wouldn't do anything in the winter anyway. I had the revision surgery on December 9, 2003--one year and one week from my resurfacing surgery--and I was surprised how easily everything went with the second surgery. For one thing, I was less nervous about the whole ordeal. Once again, I opted for general anesthesia even though they tried to talk me into having an epidural. For the resurfacing surgery a year earlier, they wanted to use general anesthesia because they wanted the muscles more relaxed, but this time I was given the option of which method I preferred. They recommended the epidural, but I stubbornly opted for the general anesthesia. I might have been less nervous this go-around, but I still did not want to be conscious during all the sawing, drilling, and hammering. After the surgery, Dr. Goldberg told me that he had been incorrect in his diagnosis of a fracture of the femoral neck. What had truly caused my problem was the development of avascular necrosis (AVN) in the femur which led to a loosening of the femoral resurfacing cap since the bone was no longer able to support it as the bone had died due to lack of blood circulation. As we had discussed before, development of AVN is still possible after hip resurfacing. My bone had become so weak and mushy at the end of the femur, that he was able to slide the femoral component out of the bone without any resistance. (Based on clinical studies, post-surgery AVN results at a rate of approximately 1 in 1000 for an incidence rate of slightly less than .1% in the resurfacing population. Similarly, 10,000 to 20,000 cases of AVN occur yearly in the general population of the U.S. for an incidence rate also less than .1%.) I asked him if my propensity to AVN should make me discount resurfacing in the future if I should need to have my other hip replaced, and he felt that it would probably be best if I opted for the large head total hip replacement instead. Perhaps my case and that of a few others will lead them to develop a test that will identify people susceptible to AVN. Although statistics don't show that people with a propensity toward AVN will definitely develop it after hip resurfacing, it could be a determining factor in the patient's decision to have the procedure. Of course, statistics show a low incidence of post-op AVN in patients in the study, and hip resurfacing is even being suggested as a treatment for younger people with AVN who still have enough healthy bone to support the femoral cap. |
|
|
January 2004 X-ray (Click on image to enlarge) |
Since my acetabular component was secure, it was only necessary to refit my femur with a Conserve Total Hip System with a large femoral head (still metal-on-metal with no polyethylene). Although the first day and night of surgery did not seem much different than the previous year, I noticed by the second day that I was in less pain and could move much easier. When they got me up and out of bed the second day, I was prepared for the excruciating pain and weakness I had experienced the previous year, but it was absent for the most part. I even managed to get back into bed myself, something I could not even have attempted after my resurfacing surgery. I attribute a lot of this to the fact that they didn't have to work on the acetabular side which would have introduce more pain and trauma into the mix. |
|
Shortly before returning to work (approximately 3 months post-surgery), I began to experience a weight-bearing ache or soreness in my thigh whenever I would start walking after sitting or lying down. Sometimes I would also experience it whenever I walked a little too far or walked too long during my therapy. I was still using a cane, but I had begun placing a lot more weight on the leg. The new pain scared me because it was very reminiscent of the soreness I first experienced when my resurfaced hip started going bad. When I mentioned the thigh soreness/ache to another THA recipient, he thought it was normal, and he suggested that it was just the femur adjusting the the new stress forces acting upon it. (I had read that the negative stress forces involved in a stemmed THA are enough to make an engineer cringe.) He likened it to "growing pains" we experienced as children as our young soft leg bones adjusted to our growth spurts and the newfound stress placed on the them. His counsel did put my mind at ease a little bit, but I was still rather paranoid after my bad experience with my resurfaced hip. I then did some research and learned of the problems of stress shielding related to the femoral stem, and it seemed to describe the discomfort I was experiencing. |
|
I had my four-month post-op visit with my surgeon on March 31, 2004. I mentioned the thigh ache/discomfort I had experienced when I began putting more weight on the leg two months earlier which had subsided but not completely vanished. He felt that stress shielding wasn't the cause, and he said that "start-up pain" experienced when I first start walking usually means that the stem has not fully seated yet. He accused me of overdoing my activity, but I thought I had been very conservative this time. I was swimming two to three times a week in addition to walking every day 20 - 30 minutes, sometimes on a treadmill. I also had only given up using a cane 3 - 4 days prior to my doctor's appointment. He said that the X-ray looked good and nothing had shifted. He advised me to continue using the cane for a while, especially whenever I experienced the thigh pain. He also told me to continue swimming and walking, but to stop walking on the treadmill. Instead, he advised using a stationary bicycle. He said that it sometimes takes a long time for the stem to solidify, and he advised me not to screw it up by overdoing it. |
March 2004 X-ray (Click on image to enlarge) |
|
Two weeks after visiting the doctor, I went on vacation. I took a trip on a cruise ship to the Caribbean, and I believe the inherent motion of the ship was good therapy. The slight roll of the ship requires you to develop "sea legs" as you constantly struggle for balance. I spoke for some time with a physical therapist onboard who was also vacationing, and she said that she'd like to be able to mimic the ship's motion for her patients. She also provided me with a lot of information about my hip restrictions after surgery. It was nice to talk to her in a relaxed manner without worrying about my appointment time running out and other patients waiting to see her. In addition to walking on the ship--and a cruise ship requires a lot of walking--I snorkeled and walked on the islands and on the beaches. All in all, the trip help restore my confidence and seemed to help strengthen my leg. I took with me a collapsible cane that I never needed to use, but at least it was there if something happened. I did set off the metal detectors at the airports that earned me closer scrutiny from the security personnel--no strip searches, just a closer examination using the metal detecting wand.. By the six-month mark, the
healing process had progress considerably although my leg did not feel
as strong as it had the previous year at the six-month mark.
The joint had become pretty limber, and I could walk without a
limp; however, stair climbing was still a slight strain on the operative
leg. In the prior month, I had
experienced three episodes of unexpected pain in my thigh that stopped
me in my tracks. The pain
began on the inside of my thigh and radiated across the entire thigh. It
was painful enough that I could not continue walking, and it was most
painful in the part of my stride where I’d bring the operative leg
forward. I feared that it
was an indication that something was wrong with the stem in the femur
(e.g. pending fracture), but then I began to believe that it was a
strain or inflammation of the muscles in the thigh. Two of the episodes happened
when I was pushing a vacuum cleaner and the third was after a day of
climbing around on my sailboat. The
pain forced me to stop what I was doing and to sit down and rest.
After I’d rise and start walking again the pain would return
after I walked a short distance. Sometimes,
if I walked very slowly, I could move without a recurrence of the pain.
Usually by the next day or the day after that, the pain would
dissipate if I took it easy and rested the leg for about a day. Since the second surgery, I
had experienced a weakness and slight soreness on the inside of the
thigh. I’d feel it
sometimes when I’d climb stairs and when I’d do my leg raising
exercises. After I
experienced a spasm of the Gracilis
muscle, I decided that the weak thigh muscles being pushed to their
limits that might have caused the episodes of pain.
(It then gave me an excuse not to run the vacuum cleaner through
my house anymore—but I still went out on my sailboat.) In June 2004, I went on vacation to the Outer Banks of North Carolina. The previous year I tried windsurfing for the first time after surgery (see windsurfing article), but I thought I’d be a little more cautious this year and skip the windsurfing. Of course, I didn’t, and I ended up windsurfing again as well as spending time in the surf riding the waves on a boogie board. However, I was very careful and cautious in the way I did all this. The hip seemed to do well on the vacation, and it wasn’t until I returned home that I started experiencing some pain. It was that same pain in my thigh that had flared up a few times in the previous two months, and it had me concerned because it was a little more intense. The "end-of-stem" pain also seemed to have increased. |
|
As it turned out, I was already scheduled to return to my surgeon for my six-month exam, and he said that everything looked good structurally. I pointed out to him a shadow at the end of the stem that seemed to indicate an area where the stem might have had some slight movement, but he said that it was not uncommon there because, in the center of the femoral canal, there is really nothing to grip onto the stem. It is just bone marrow that has the structural strength of dry wall. |
June 2004 X-ray (Click on image to enlarge) |
|
(Click on image to enlarge) |
I did have some additional development of free floating bone growth in the soft tissue around the hip (i.e. heterotopic ossification)—a common occurrence in males after joint replacements—with an especially long piece growing in the tissue on the inside of my thigh. Dr. Goldberg speculated that this bone might be irritating the muscle when I move certain ways and causing the discomfort I sometimes felt on the inside of my thigh. Since the bony growths were not interfering with the movement of the joint, he said not to worry about them. He also told me to continue swimming, walking, and bicycling in order to strengthen the leg. |
|
Since my insurance company wanted my care administered by an in-network surgeon, Dr. Goldberg released me from his care after my six month visit as he had promised. I scheduled an appointment for the beginning of August 2004 with Dr. Ernest Swanson in Sharon, Pennsylvania (only 20 miles from my home) in order to continue my care. I chose Dr. Swanson, not only because of his close proximity to me, but because he and Dr. Goldberg know each other and because Dr. Swanson is affiliated with Wright Medical Technologies, the manufacturer of my hip implant. |
| My visit with Dr. Swanson was very enjoyable. He allotted me more of his time than I think any doctor has ever given me. He also pointed out that he is a former student of Dr. Goldberg. I provided him with Dr. Goldberg's physician notes along with digital images of all my X-rays dating back to 1998. He reviewed everything and examined me, and then he spent a considerable amount of time talking to me and answering all my questions. He also pointed out that my left hip now has no internal rotation, which is less rotation than my right hip had before surgery according to Dr. Goldberg's notes, but as he pointed out, "If it don't hurt, don't fix it." |

August 2004 X-ray (Click on image to enlarge) |
|
We spent time examining the new X-rays that were taken that day. He said that the heterotopic bone growth had not increased any since the last X-ray, and the edges of the heterotopic bone seem smooth. He doubted that it should be causing me any pain. He pointed out the shadow at the tip of the stem, which he referred to as a "windshield wiper" effect, and said that it indicated some slight movement that had taken place earlier in my recovery. He also went onto explain how it can happen and how various prosthesis manufactures try different stem designs in an effort to combat it. Since the movement was not indicated farther up the stem where the femoral component is anchored, he said it should not be a problem; however, it may cause me some intermittent thigh pain. Dr. Swanson traced around the prosthesis with his finger to show the jagged appearance of the contour indicating bone in-growth. It was only near the edge of the acetabular cup where a tiny space could be detected, but he said that the space was insignificant. He pointed out that surgeons try to get things right the first time because a revision is never as good as the original hip replacement. But if he had to grade my hip revision, he said he'd give it an A--not an A+ only because I was experiencing some occasional thigh pain that he attributed to "windshield wiper" effect at the end of the stem. He said that the gap might fill in over time and the pain would vanish, or things might remain unchanged and the intermittent thigh pain might linger and become something that I had to live with. I asked Dr. Swanson if he had any other patients who had received the Conserve Total Hip System with BFH Technology, and he said, "No." He said that he used Wright Medical Technology equipment, but he was implanting mainly ceramic hips at that time. He directed his staff to make copies of my X-rays and send them to Dr. Goldberg, and he composed a letter about my examination to accompany the X-rays. Because Dr. Swanson has not had any direct experience with the Conserve Total Hip System, it made be feel better knowing that he was keeping Dr. Goldberg updated and informed of my progress in the event future complications develop. He told me to return in December 2004 for my one-year follow-up exam. Like Dr. Goldberg, he felt that the surgery was successful and didn't foresee any problems. I was instructed to continue exercising and strengthening the hip. The day before my exam, I had shoveled and spread 10 1/2 tons of topsoil which I guess is a testament to the success of the surgery. However, a two weeks after my exam I took a long hard fall off my boat and landed on my tailbone, which gave me a real scare. At the same time I had another scare when I learned that Wright Technologies were recalling some of the acetabular cups because of a defect, but I then learned that I had not received one of the defective cups. |
|
|
December 2004 X-ray (Click on image to enlarge) |
I made it through the summer and returned to Dr. Swanson in December 2004. Throughout the summer, I had some aching in the hip now and then, but the hip slowly strengthened. By the time December rolled around, I could climb stairs without any strain felt in the hip. (It had taken only 8 months to reach that point the previous year.) Dr. Swanson again thought the X-rays looked great, and he told me I didn't have to return for a year. As for some of the aches and pains I'd sometimes experience, he really couldn't explain. He said the implant looked really well seated and stable, and the heterotopic bone growth appeared to have halted. He again traced over the X-ray to show all the bone growth and the positive stress/load indications. He said he could see the implant lasting 25 years even though he said he didn't want to jinx me by saying that. |
| In looking at the X-rays, he said that he thought the "windshield wiper effect" at the end of the stem was filling in a little, but I couldn't notice the difference (see below). All in all, it was a good visit, and it gave me more confidence. My only complaint was pain in my knee. When it first started a few days before my doctor's visit, I panicked because referred pain in my knee was one of the indicators of my loose femoral cap the previous year; however, the pain was much greater then. After some research, I determined that it was illiotibial band syndrome (ITBS) because the pain matched exactly the ITBS symptoms, and my incision is very tight and directly over the IT band. It seems to shorten the IT band and cause friction on the outside of my knee. By doing exercises that stretched the band, I am able to alleviate most of the discomfort. | |
|
August 2004 X-ray (Click on image to enlarge) |
December 2004 X-ray (Click on image to enlarge) |
|
I returned in December 2005 for my yearly X-ray and follow-up exam. The X-ray looked unchanged, and the implant appeared to be fixed solidly. No change was detected in the heterotopic ossification that was seen in the current and previous X-rays. For the first time I got to hold and examine an actual metal-on-metal head and acetabular socket like the one I had. I was amazed how heavy it was. Just the head and socket weighed as much if not more than the traditional THA implant that Dr. Swanson also showed me. I was also impressed at how the metal surfaces glided freely against each other. The demo implant was scratched considerably, and still the surfaces glided smoothly. He also demonstrated how hard it would be to dislocate the large metal-on-metal head as opposed to the traditional head. |
|
| I asked him if it
would be okay to put my ankle across the opposite knee in order to
put on and tie my shoes. It had begun to hurt my lower back
trying to reach down to my foot as if I was pinching a
nerve.
Dr. Swanson said it would be okay to do it, but I was so tight (and a little gun-shy) after not having done it for many years, that I couldn't do it. He told me to slowly try to lift the ankle over time until I was able to get it on the knee. He still recommended that I not cross one knee over the other, but I've never been able to do that my entire life. He also said that it is good for the muscles to be a little tight around the hip. Problems of dislocation arise when things get too loose, which is why I could never understand other hip replacement patients trying to stretch their muscles and tendons in order to become real flexible again. I think that just leads to trouble down the road, and the doctor seemed to agree. |
December 2005 X-ray (Click on image to enlarge) |
|
Besides giving me the green light to bring my
leg over my knee, Dr. Swanson also said that I could resume
weightlifting if I wanted to and that I should carry on with my
regular activities without fear. Over the past year I had
chartered a boat in the British Virgin Islands, and I cruised single-handedly
for a week on my boat in the Chesapeake. Both of those are
things I plan to continue. I didn't windsurf or play golf over
the past year, only because the circumstances didn't present
themselves; however, I intend to do so again this coming summer.
It really seemed that it took two years to reach this point in the recovery process. Maybe it's because of the two surgeries that it took two years to recover, or maybe I'm just a slow healer. I noticed over the year that the hip needs rest. If I don't get enough sleep, my hip will be a little tender the next day. I've come to liken a hip replacement to this: It's like getting the hip of a healthy 65-year-old. If you're 95 when you get it, you think it's great. However, if your 35 when you get it, you might think it's a little restrictive. After all, a normal, healthy 65-year-old can walk, dance, play golf, but he's usually not out there playing football, soccer, or rugby. It's just a matter of adjusting your lifestyle a little--not a lot, but a little. |
|
|
I did not return to the doctor at my three-year anniversary in December 2006 because he told me to wait until 18 months after my last visit in December 2005. Except for a few episodes of soreness now and then, my third year was the best. The hip felt much stronger, and I attempted more aggressive activities--like reinforcing my porch and putting on a new porch floor by myself. While on vacation in November, I even ventured onto a sand volleyball court for a short game. It was difficult to keep from reverting to my former style of play, but I managed to curb my enthusiasm and not dive for the ball or jump at the net. I played terrible, but it was rejuvenating just to be out on the court again--a return to the scene of the crime since it was a volleyball injury that initiated the downfall of my hip joint. |
|
|
June 2007 X-ray (Click on image to enlarge) |
I returned to the doctor in June 2007 for a
check up. Once again he said everything looked good, and I had
to admit that the hip felt better than it ever had. I had gone
windsurfing once during the summer, and I was amazed at the
flexibility I had regained. Rising on the board was effortless
where it had still be a slight challenge even a year earlier.
Everything was looking up. Then in early September I played golf for the first time in five years. I hadn't swung a club since prior to my first surgery, but I went out and played 18 holes in an executive golf outing. As it happened, I found myself limping by the end of the round, and after several weeks, I was still getting a dull ache in my thigh when I walked. I was afraid that the swinging of the golf club and the twisting of my body had disturbed something. It was a familiar pain--almost like end-of-stem pain--that I had felt before but not for several years. I prayed that my golfing activities hadn't caused a loosening of the stem. Eventually, I went back to my surgeon to get his opinion. After a new X-ray and examination, he decided that it was probably just a muscular injury caused by golfing. We both decided that it would be best if I refrained from that sport. |
| Shortly afterwards, I went on a cruise vacation and my hip did just fine. It was still a little sore but it eventually strengthened due to all the walking I did on vacation. My cabin was on the first level and I continually walked the stairs up and down to the 12th deck. It really seemed to do my hip good and it helped to alleviate my fears. The whole episode did remind me how fast things can turn around and it helped remind me to be careful so I can avoid a return trip to the operating room. | |
|
Late November 2008 I returned to the original doctor who performed my surgeries, Dr. Goldberg, because the doctor who I had been using to monitor my progress, Dr. Swanson, planned to retire in December. I wanted to ensure some continuity with a surgeon who used Wright Technology equipment, so I again sought out Dr. Goldberg. My insurance then extended its network nationwide, so the roadblock to returning to Cleveland, Ohio, for my treatment was removed. By then Dr. Goldberg had stopped performing operations but was still consulting and following up with his patients. He told me that he had a lot of his former students on staff who were excellent surgeons in the event something happened that called for surgery. About ten days earlier I had started experiencing some discomfort in my hip, but based on my complaints and the X-rays, he determined that it was probably just some bursitis that had flared up. Otherwise, everything looked good and he told me to continue as I had been doing. Earlier in the year I had been diagnosed with spinal stenosis and had undergone spinal decompression surgery on my cervical spine (see the spinal stenosis page). Since I had read that orthopedic surgeons also perform anterior cervical discectomy with fusion and plating surgery, I took my MRI and X-rays to get his opinion of the work that was done on me. He was quick to point out that my three month X-ray revealed that it was not healed at the time and he strongly suggested that I have another X-ray taken since it had been eight months from the surgery. His multiple suggestions that I have another X-ray taken made me a little paranoid--actually I had been paranoid since I had the surgery--so I determined to contact the neurosurgeon on my return home and insist that he follow-up with me and order a new X-ray. |
|
|
Although it was disappointing having to go through hip surgery and recovery a second time back in 2003, I'm still glad I gave hip resurfacing a try. Had I not done so, I always would have questioned my decision. I would still prefer to have a resurfaced hip, but at least I received the next best thing. Although my actions are slightly limited compared to resurfacing (e.g. no competitive volleyball in my future), at least I am better off than a traditional THA because the large femoral head of the Conserve Total reduces much of the dislocation risk (e.g. I'm still able to windsurf). The one side benefit is that the Conserve Total Hip System with BFH Technology offers the greatest range of motion of all the hip systems (i.e. traditional THA and resurfacing) because the ratio of the size of the head to the width of the neck is the greatest, and the hip can rotate farther before the neck impinges on the side of the acetabular cup and "levers out" the femur component, causing a dislocation. See, I guess there was a silver lining to the dark cloud I experienced. |
|
|
As an aside, what are the odds that my dog--a 5-year-old Beagle named Mulder--would develop mild hip dysplasia, mainly of the right hip just like mine? I noticed him limping a little during the winter while I recovered from my second surgery. By summer, he was having problems jumping up onto the bed and the seat of my truck. He also began taking stairs one step at a time. Getting on his feet after lying down had started giving him some problems, so I took him to the vet.. When his hips were X-rayed, it showed that his femurs were slightly irregular (especially the right hip) with some mild flattening. It was diagnosed as mild canine hip dysplasia. I've heard of people starting to look like their pets, but this is ridiculous. |
August 2004 Canine X-ray (Click on image to enlarge) |
|
If you are thinking about having hip resurfacing or hip replacement surgery and you have any questions, feel free to call or email. |
![]()
Jamaican Farewell available at JamaicanFarewell.com
jkwaltenbaugh@BananaRepublican.us
| Photo Gallery | Opinion Column | US Constitution | BVI Tours | Lake Arthur | Banana Wind | Spinal Stenosis | Hip Surface Replacement | Waltenbaugh.net |
Last update: Tuesday, February 13, 2024



























.jpg)

